


Lucie Culver, Jeffrey W. Imani-Eaterry, Lorraine Sherr, Mary Mahy, Seth Flaxmen.
Published August 17, 2023, The Lancet
As researchers on HIV, AIDS, and paediatric health, nothing is more central to our work than preserving children’s lives. Considering the current challenge to the 5-year reauthorisation of the US President’s Emergency Plan for AIDS Relief (PEPFAR), we used 2023 UNAIDS estimates on the prevalence of children orphaned by AIDS, infant and young child HIV- infections, and incidence of adult and child AIDS deaths to estimate PEPFAR’s effect on child survival and health. We focused on sub-Saharan Africa: the region receiving more than 90% of PEPFAR funds and containing two-thirds of all people with HIV. We note that PEPFAR provides support through and in partnership with the Global Fund to Fight AIDS, Tuberculosis and Malaria (to which PEPFAR is the largest donor), national governments, UNAIDS, and other UN agencies.
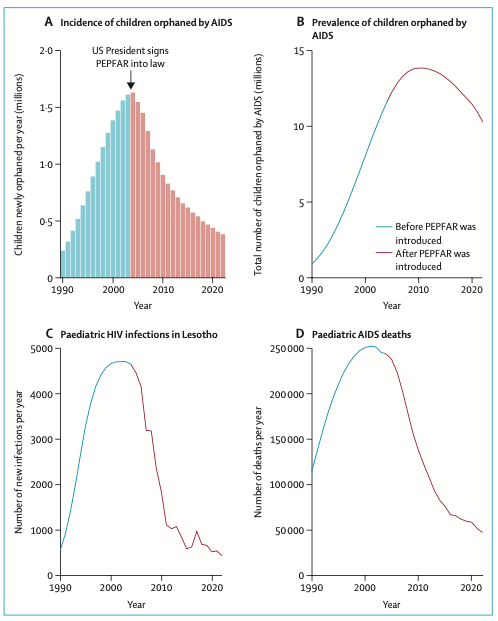
Figure: AIDS orphanhood, infant and young child HIV infections, and infant and young child AIDS deaths in sub-Saharan Africa
(A) Incidence of orphanhood caused by AIDS in sub-Saharan Africa (children aged <18 years who are newly orphaned per year). Regression model estimates were based on linear regression with no intercept term, 1-year lagged orphanhood prevalence, and new AIDS deaths for individuals aged 15–49 years, based on UNAIDS data. (B) Prevalence of orphanhood caused by AIDS in sub-Saharan Africa (living children
[aged <18 years] who were orphaned by the loss of at least one parent). Replication code is available at https://github.com/MLGlobalHealth/PEPFAR-letter. (C) New HIV infections due to vertical transmission (infants and young children aged <36 months) in Lesotho, 1990–2022, based on UNAIDS data. (D) Paediatric AIDS deaths in sub-Saharan Africa, based on UNAIDS data (infants and young children aged <36 months).
PEPFAR has substantially reversed the devastating effects of HIV and AIDS on children who are newly orphaned (figure A). Loss of a parent is associated with education loss, child abuse, and child sexual exploitation, with consequent elevated risks of HIV infection. Using UNAIDS data, we estimated the number of children who were newly orphaned by AIDS annually before and after PEPFAR by regressing orphanhood prevalence on previous-year orphanhood prevalence and adult (aged 15–49 years) AIDS deaths. Incidence of orphanhood in sub-Saharan Africa increased rapidly from 1990, reaching a peak of 1.6 million children newly orphaned by AIDS (aged <18 years) during 2004. In this year, PEPFAR began to prevent parental deaths via a massive roll-out of antiretroviral agents to 28 countries in sub-Saharan Africa. From 2005, the incidence of orphanhood due to AIDS has reduced annually to 382,000 in 2021.
UNAIDS data show that 10.3 million children orphaned by AIDS in sub-Saharan Africa remain in need of support (figure B). Globally, 13.9 million children are orphaned, living without one or both parents who have died of AIDS, alongside 7.5 million children orphaned due to COVID-19-associated excess deaths. 10% of PEPFAR’s bilateral funding is dedicated to care of orphaned and vulnerable children, including provision of nutritious food, school fees, small loans and savings clubs for caregivers, and psychosocial support. Failure to reauthorise PEPFAR would mean that this support will no longer be guaranteed.
The PEPFAR era has brought four-fold reductions in new HIV infections among infants and young children. PEPFAR reduces paediatric infections through programmes for prevention of parent-to- child transmission, and through antiretroviral agent roll-out, which suppresses viral load and therefore the transmission of HIV to partners and children. New HIV infections among infants and young children (aged <36 months) in sub-Saharan Africa escalated from 250,000 in 1990 to more than 465,000 per year between 1999 and 2002, then reduced to 110,000 by 2022. As an example, figure C shows incident HIV infections in infants and young children in Lesotho. We saw rapid reductions in paediatric infections in the PEPFAR era, despite increasing numbers of women with HIV: 4,600 children were infected per year in 2004, which reduced to fewer than 500 per year in 2022.
Since PEPFAR’s implementation, AIDS deaths in infants and young children have fallen by 80% (figure D). Using the UNAIDS data, we examined deaths among infants and young children from 1990 to 2022. PEPFAR prevents child deaths by preventing infections and providing antiretroviral agents to children born with HIV—without which 50% of infants will die before reaching 2 years of age. Figure D shows that deaths among infants and young children in sub-Saharan Africa more than doubled during the 1990s, reaching 240,000 per year in 2004. After PEPFAR implementation deaths reduced five-fold to 47,000 in 2022.
PEPFAR has supported 7.1 million children who are orphaned and vulnerable and their caregivers, and provides 700,000 children per year with antiretroviral medication and psychosocial and nutritional support to stay on treatment. PEPFAR’s direct effects extend further to the reduction of subsequent negative outcomes on children’s lives, such as avoidance of HIV- related developmental delays, family breakdown and separation, abuse and mental health distress, and reduction of poverty-driven sexual exploitation of children.
But the task is far from done. During COVID-19 lockdowns, PEPFAR innovated to provide continuity of HIV care and child abuse prevention, but the initiative now needs to develop preparedness for future pandemics. Only 56% of children aged younger than 14 years with HIV in sub-Saharan Africa have access to antiretroviral treatment. Prevention of parental and child deaths requires sustained provision of antiretroviral medication and prevention of parent-to-child transmission. PEPFAR is working, where feasible, to support sustainable shifts towards national government ownership of antiretroviral programmes, but evidence shows that successful transitions require planning and investments in national financial, technical, and logistical capacity. Abrupt halting of development aid can cause health system collapses. PEPFAR, the Global Fund to fight AIDS, Tuberculosis and Malaria, national governments, and donors such as the Bill & Melinda Gates Foundation are a crucial partnership for global health security.
In 2022, PEPFAR provided life-saving antiretroviral medication to 20 million people—most of them parents and children. Epidemiological models for children younger than 15 years predict that a 6-month interruption in supply would cause an additional 107 300 paediatric HIV infections and an additional 20 600 childhood AIDS deaths within a year.
Loss of PEPFAR would inevitably result in death, orphanhood, and suffering for millions of children.
Further Information
For PEPFAR’s legislative background see https://sgp.fas.org/crs/misc/IF12463.pdf
For 2023 UNAIDS estimates see https://aidsinfo.unaids.org
For more on global resources for the HIV/AIDS epidemic see https://www.kff.org/global-health-policy/fact-sheet/the-global-hiv-aids-epidemic
For more on what PEPFAR has supported see https://www.state.gov/wp-content/uploads/2022/05/PEPFAR2022.pdf
For further results attributed to PEPFAR see http://www.miriamzoll.net/documents/ USAID-PEPFAR%20OVC%20Eval.pdf
Recognition
LC declares research grants to her institutions from UK Research and Innovation, UNICEF, European Research Council, Wellspring Philanthropic Fund, the LEGO Foundation, the Global Fund to Fight AIDS, Tuberculosis and Malaria, a private family foundation that wishes to remain anonymous, and UK Medical Research Foundation; LC also received a consultancy from the Unified Budget, Results and Accountability Framework. JWI-E declares research grants to his institutions from UK Research and Innovation, the National Institutes of Health, Bill & Melinda Gates Foundation, UNAIDS, and WHO; and received a consultancy from Oxford Policy Management and a consultancy to his institution from BAO Systems. LS declares research grants to her institution from UK Research and Innovation. SF declares research grants to his institution from UK Research and Innovation, the US Centers for Disease Control, and WHO; and a consultancy from WHO. MM declares that UNAIDS receives funding from the US President’s Emergency Plan for AIDS Relief and from the Bill & Melinda Gates Foundation, among other funders. All authors had full access to all the data and had final responsibility for the decision to submit for publication. All data is available on the UNAIDS website or from UNAIDS Data for Impact Practice. For any requests for data, please contact aidsinfo@unaids.org.
*Lucie Cluver, Jeffrey W Imai-Eaton, Lorraine Sherr, Mary Mahy,
Seth Flaxman lucie.cluver@spi.ox.ac.uk
Department of Social Policy and Intervention (LC) and Department of Computer Science (SF), University of Oxford, Oxford, OX1 2ER, UK; Department of Psychiatry and Mental Health, University of Cape Town, Cape Town, South Africa (LC); Center for Communicable Disease Dynamics, Department of Epidemiology, Harvard T H Chan School of Public Health, Harvard University, Boston, MA, USA (JWI-E); MRC Centre for Global Infectious Disease Analysis, School of Public Health, Imperial College London, London, UK (JWI-E); Institute for Global Health, Faculty of Population Health Sciences, University College London, London, UK (LS); Data for Impact, UNAIDS, Geneva, Switzerland (MM)
Footnotes
1 Diamond D. Lifesaving HIV program faces a new threat: US abortion politics. 2023. https:// www.washingtonpost.com/ health/2023/07/29/pepfar-aids-hiv-abortion- congress/ (accessed July 30, 2023).
2 Operario D, Underhill K, Chuong C, Cluver L. HIV infection and sexual risk behaviour among youth who have experienced orphanhood: systematic review and meta-analysis. J Int AIDS Soc 2011; 14: 25.
3 Hillis S, N’konzi JN, Msemburi W, et al. Orphanhood and caregiver loss among children based on new global excess COVID-19 death estimates. JAMA Pediatr 2022;176: 1145–48.
4 Newell M-L, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV- infected mothers in Africa: a pooled analysis. Lancet 2004; 364: 1236–43.
5 Holtzman CW, Godfrey C, Ismail L, et al. PEPFAR’s role in protecting and leveraging HIV services in the COVID-19 response in Africa. Curr HIV/AIDS Rep 2022; 19: 26–36.
6 Huffstetler HE, Bandara S, Bharali I, et al. The impacts of donor transitions on health systems in middle-income countries: a scoping review. Health Policy Plan 2022; 37: 1188–202.
7 Stover J, Glaubius R, Teng Y, et al. Modeling the epidemiological impact of the UNAIDS 2025 targets to end AIDS as a public health threat by 2030. PLoS Med 2021; 18: e1003831.
8 Chun HM, Dirlikov E, Cox MH, et al. Vital signs: progress toward eliminating HIV as a global public health threat through scale-up of antiretroviral therapy and health system strengthening supported by the US President’s Emergency Plan for AIDs Relief—worldwide, 2004–2022. MMWR Morb Mortal Wkly Rep 2023; 72: 317–24.
9 Flanagan CF, McCann N, Stover J, Freedberg KA, Ciaranello AL. Do not forget the children: a model-based analysis on the potential impact of COVID-19-associated interruptions in paediatric HIV prevention and care. J Int AIDS Soc 2022; 25: e25864.
